IBD Academy: Treatment with Immunomodulators and Biologics
IBD | Information
We’ve arrived at the heavy hitters! Going back to the first installment of IBD Academy (“Back to Basics”), remember that inflammatory bowel disease is fundamentally an autoimmune disorder in which the immune system mistakingly attacks the body’s own tissue. To inhibit and counteract this reaction, immunomodulators and biologics are used to dampen the autoimmune response. A serious concern in using these medications is that T lymphocytes, the white blood cells at the center of autoiummunity, are widespread in the body. Targeting them induces to systematic, not local, immunosuppression, meaning that the gut isn’t the only part of the body affected. Regular blood tests are usually done to check liver, kidney, and bone marrow function because of the suppressive effects that these drugs have on the immune system. Patients on immunomodulators and/or biologics are also encouraged receive yearly flu vaccines and avoid live vaccines while on these medications. Because there are so many cells and molecules involved in autoimmunity, here are some key players to familiarize yourself with and refer back to while diving into the mechanisms utilized by various immunosuppressant medications.
KEY Vocab
intestinal mucosa: the tissue that lines the GI tract and is made up of endothelial cells
attacked by white blood cells in the autoimmune reaction that is the basis of IBD
T lymphocyte or T cell: a type of white blood cell central to the immune response in IBD and other autoimmune disorders
antibody: proteins that circulate in the blood following their production by the immune system in response foreign particles detected in the body
may be produced by the body or created artificially to be used as a drug
cytokine: signaling proteins essential for communication between cells involved in the inflammatory response (may be pro-inflammatory or anti-inflammatory)
interleukin: a class of cytokines involved in modulation of immune responses and the development of T lymphocytes
TNF-α (tumor necrosis factor alpha): a pro-inflammatory cytokine and central regulator of immune function that is the target for multiple biologic therapies for autoimmune disorders
α4β7 integrin: a receptor on T cells that allow them to interact with other cells in the body
MAdCAM-1: a protein expressed on the endothelial cells of small blood vessels in the intestinal mucosa
Immunomodulators
drugs that modulate and/or weaken the immune system in order to dampen the inflammatory response
may be used in conjunction with a biologic (“dual therapy” or “combination therapy”) to increase the chance of inducing and maintaining remission
Thiopurines
azathioprine (Imuran): oral
6-mercaptopurine (6-MP, Purinethol): oral
mechanism of action: prevents the activation of T lymphocytes, which keeps them from attacking the intestinal mucosa and causing inflammation
may take three months to work; therefore, patients are often on steroids until the new medication kicks in
methotrexate: subcutaneous (SC) injections
mechanism of action: in addition to acting at a cellular level like thiopurines, methotrexate may also inhibit pro-inflammatory cytokines like IL-1 (interleukin-1) and TNF-α in the bloodstream
traditionally used to treat rheumatoid arthritis or lupus, it can be used in Crohn’s patients who have failed or become tolerant of thiopurines
hasn’t been shown to be effective in UC
must be used with caution in women of child-bearing age due to the risk of birth defects or miscarriage
cyclosporine: oral
mechanism of action: prevents T lymphocytes from producing cytokines or multiplying
traditionally used to prevent rejection following an organ transplant, it can be used for patients with severe UC
much more rapid onset of action than thiopurines (takes 1-2 two weeks to begin working)
tacrolimus: oral or topical
mechanism of action: also prevents T lymphocytes from making cytokines or multiplying
traditionally used to prevent rejection following an organ transplant, it can be used for patients with severe UC or fistulizing Crohn’s
can be used topically for active Crohn’s disease around the mouth or perianal area and on the skin for pyoderma gangrenosum
Biologics
drug names end in “mab”, which stands for monoclonal antibody
biologics are antibodies designed to bind to and inhibit inflammatory factors or other molecular targets involved in the immune response in IBD
because antibodies are foreign proteins, the immune system can then produce anti-drug antibodies against the biologic itself, causing the drug to stop working
many IBD patients switch to another biologic after forming antibodies against one
listed below in order of FDA approval (oldest to newest)
Anti-TNFs
mechanism of action: bind to block excess TNF-α in the bloodstream in order to prevent it from attacking healthy cells in the gut (see figure below)
Remicade (infliximab): infusion every 8 weeks
FDA approved to treat Crohn’s disease and ulcerative colitis in adults and children
two biosimilars, essentially a “generic” are now available
Renflexis (infliximab-abda) and Inflectra (infliximab-dyyb)
also treats rheumatoid arthritis, plaque psoriasis, psoriatic arthritis, and ankylosing spondylitis
Humira (adalimumab): SC injection every 2 weeks
FDA approved to treat Crohn’s disease in adults and children and ulcerative colitis in adults
also treats juvenile and adult rheumatoid arthritis, plaque psoriasis, psoriatic arthritis, ankylosing spondylitis, hidradenitis suppurativa, and panuveitis
Cimzia (certolizumab pegol): SC injection every 2 weeks
FDA approved to treat Crohn’s disease in adults
also treats rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis
Simponi (golimumab): SC injection every 4 weeks
FDA approved to treat ulcerative colitis in adults
also treats rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis
indicated for patients who have not responded to or lost response to an anti-TNF
Tysabri (natalizumab): infusion every 4 weeks
mechanism of action
binds to the α4β7 integrin receptor on T cells and blocks their interaction with the MAdCAM-1 protein on blood vessels in the intestinal mucosa
prevents T cells from migrating from the blood stream to attack the intestinal mucosa
also blocks T cell interaction with the VCAM-1 protein on endothelial cells elsewhere in the body
associated with an increased risk of a rare brain infection called progressive multifocal leukoencephalopathy (PML), especially if used in conjunction with another immunosuppressant drug
FDA approved to treat adult Crohn’s disease
also treats multiple sclerosis
Entyvio (vedolizumab): infusion every 8 weeks
mechanism of action
also binds to the α4β7 integrin receptor on T cells to block their interaction with MAdCAM-1, preventing T cell migration into the gut
doesn’t affect VCAM-1 and has not been shown to cause PML
the first and only current biologic that targets a “gut-focused” inflammatory pathway
FDA approved to treat adult Crohn’s disease and ulcerative colitis
because it targets a gut specific inflammatory mechanism, it’s used exclusively for IBD
Anti-interleukin
Stelara (ustekinumab): SC injection every 8 weeks
mechanism of action
targets proinflammatory factors IL-12 and IL-23 (interleukins) to prevent them from activating T lymphoctyes
FDA approved to treat adult Crohn’s disease
also treats plaque psoriasis and psoriatic arthritis
*Notes: Dosing listed is baseline guidelines for each medication following the induction stage of treatment. Based on an individuals response, the schedule may be adjusted for more frequent dosing.*
No individual or class of biologics has been shown effective in treating most cases of IBD. It is currently unknown why a given patient will respond to one biologic and not another. Because the series of molecular interactions that lead to active IBD (the “inflammatory cascade”) is a complicated web of triggers and interactions, there are many, many, potential molecular targets for new treatments. In addition to targeting pathways common to many autoimmune disorders, researchers are also attempting to develop new biologics with gut-specific mechanisms of immunosuppression, such as that of Entyvio. Medications that work this way are safer overall in that they suppress the immune system in a more local manner, making patients less susceptible to certain infections in comparison to those on older, more general immunosuppressants.
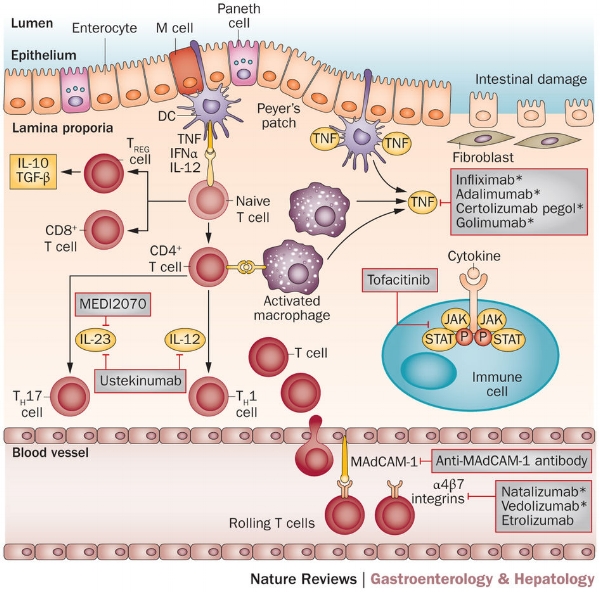
The immune response leading to intestinal inflammation in active inflammatory bowel disease consists of a variety of pro-inflammatory factors, including the cytokines TNA-α and interleukins, as well as the activation of multiple types of white blood cells (mainly various T cells). Each of these molecules and associated cell receptors represent potential targets for IBD therapies. The top section of this figure shows targets and associated drugs in the intestinal mucosa (anti-TNFs and anti-interleukins). The bottom section shows targets in the bordering blood vessels (anti-integrins). Image taken from Danese, S., Vuitton, L., and Peyrin-Biroulet, L. Biologic agents for IBD: practical insights. Nature Reviews Gastroenterology & Hepatology 12, pages 537–545 (2015). doi:10.1038/nrgastro.2015.135.
WHILE WE STRONGLY ADVOCATE BEING INVOLVED IN DECISIONS REGARDING YOUR TREATMENT, MAKE SURE THAT YOU ONLY TAKE MEDICATIONS AS PRESCRIBED BY YOUR DOCTOR AND UNDER HIS/HER SUPERVISION.
Coming up next is IBD Academy: Surgery and Ostomies.
Danese, S., Vuitton, L., and Peyrin-Biroulet, L. Biologic agents for IBD: practical insights.
Kristen Weiss Sanders is a proud ostomate and third generation girl with guts diagnosed with IBD in 2004. She is passionate about patient education and encourages those with chronic illness to be a knowledgable part of their healthcare team. Kristen credits the constant example and support of the strong women in her family for her determination to thrive with Crohn’s disease and use her IBD journey to empower others.